")
Two clinics can hire the same nurse practitioner with the same credentials—and operate under completely different legal rules.
Not because one clinic is doing something wrong, but because the state they operate in defines authority differently.
That’s the reality of full practice authority (FPA). In some states, nurse practitioners can practice independently. In others, they cannot. For healthcare clinics, that difference affects staffing models, supervision requirements, documentation, and long-term compliance strategy—especially when viewed alongside how nurse practitioner scope of practice differs by state.
Who Needs to Be Paying Close Attention to This
If you own or operate a healthcare clinic that employs nurse practitioners, full practice authority laws already shape how your clinic functions.
This applies across primary care, specialty clinics, outpatient settings, and multi-location practices. It matters even more for clinics expanding into new states, redesigning care teams, or trying to improve access while managing physician workload.
Full practice authority doesn’t just affect providers—it affects the entire clinic structure.
What This Means for Clinic Owners
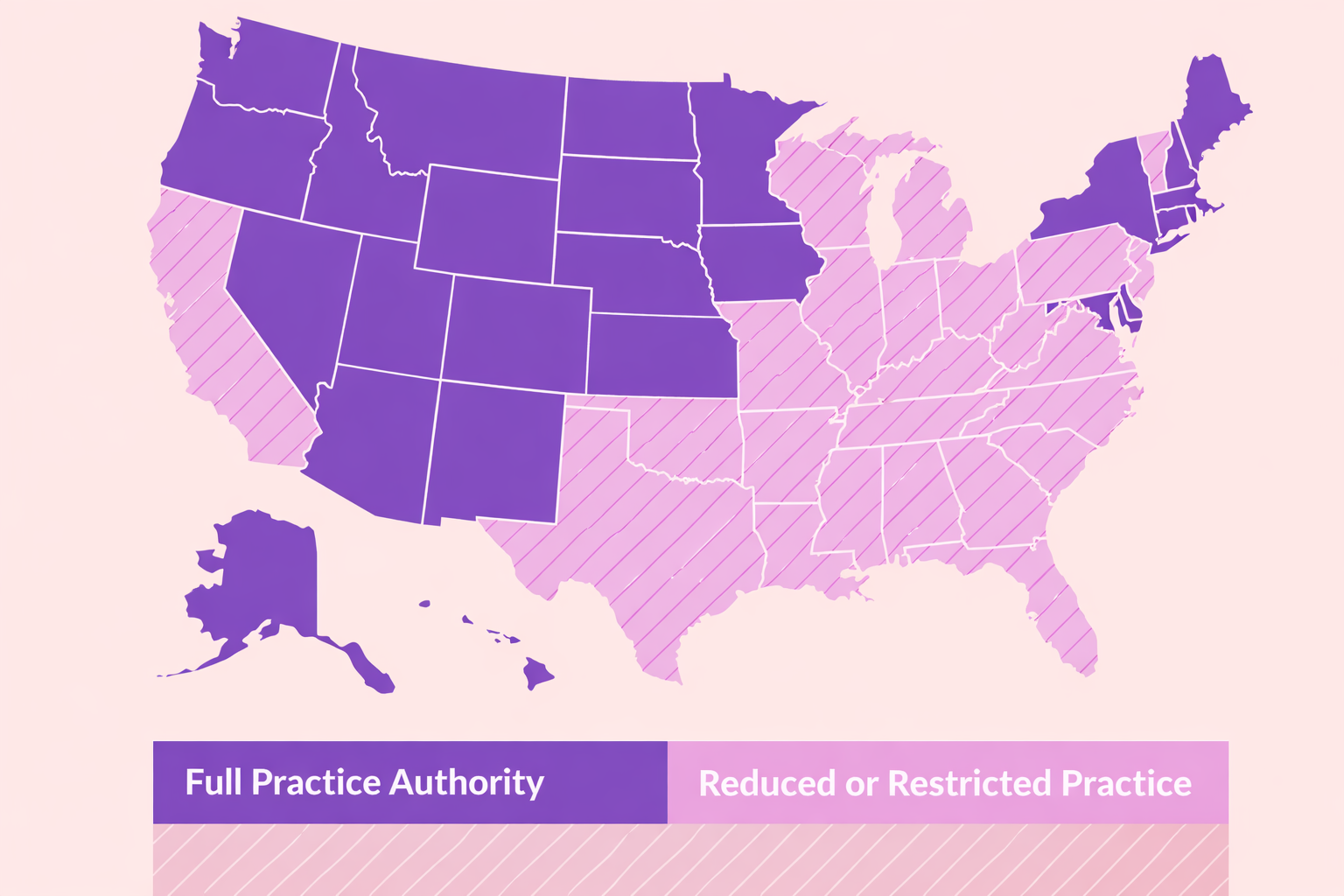
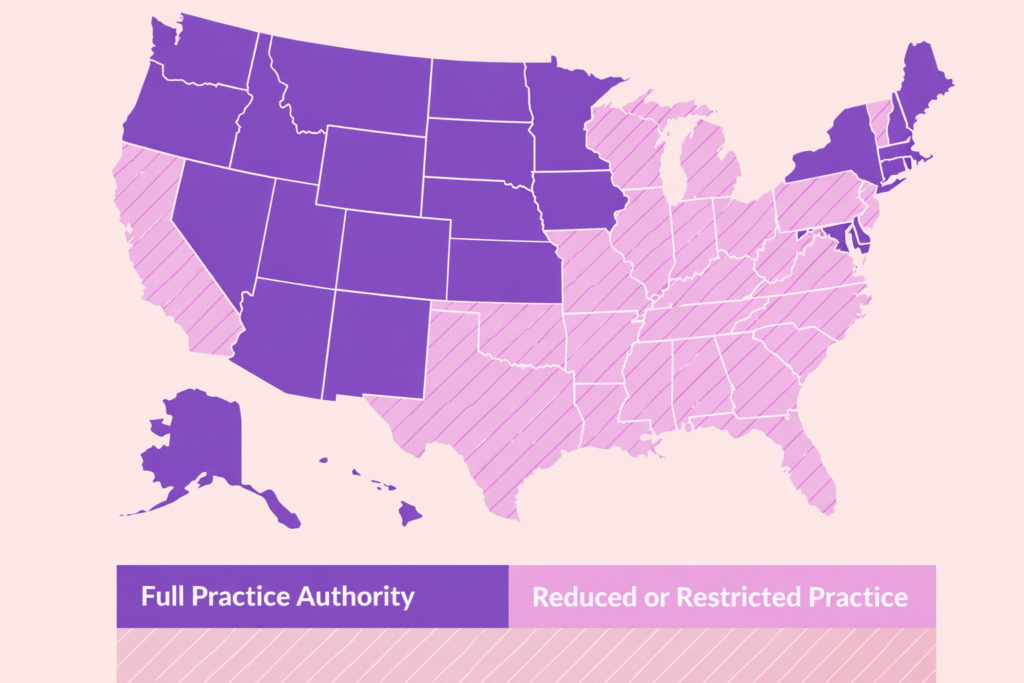
Full practice authority determines whether nurse practitioners may evaluate patients, diagnose, treat, and prescribe independently under state law.
In full practice authority states:
- NPs practice under their own license
- Physician supervision or collaboration is not legally required
- Clinics have more flexibility in staffing and delegation
In non-FPA states, clinics must account for supervision agreements, documentation requirements, and oversight structures that are enforced through licensing boards and audits.
Understanding official state-by-state full practice authority classification is essential because clinics are evaluated on legal authority—not operational intent.
What “Full Practice Authority” Actually Means
Full practice authority is not a clinic policy. It is a statutory framework set by state law.
States with FPA allow nurse practitioners to:
- Provide patient care independently
- Prescribe medications within the scope of state law
- Be accountable to the nursing board rather than physician oversight
States without FPA fall into reduced or restricted practice models, which impose varying degrees of physician involvement.
These distinctions are grounded in state legislative frameworks for scope of practice laws, not professional preference.
Why Clinics Get This Wrong
Many clinics assume that full practice authority automatically simplifies compliance.
It doesn’t.
While FPA removes mandatory physician supervision, clinics are still responsible for:
- Credentialing and privileging
- Scope alignment within clinic policies
- Billing and payer compliance
- Risk management and documentation
Full practice authority expands flexibility—but it does not eliminate regulatory responsibility.
This is where clinics benefit from designing compliant clinic structures that reflect both state law and operational reality.
Staffing Flexibility vs. Structural Risk
In FPA states, clinics often move quickly to redesign staffing models.
That can be a strength—but only when authority, accountability, and documentation are clearly defined. Clinics that treat FPA as “hands-off” risk creating gaps between provider independence and clinic governance.
Professional guidance on nursing regulation and scope of practice standards makes clear that independence does not remove the clinic’s obligation to ensure lawful practice.
Why State Lines Matter More Than Clinics Expect
A nurse practitioner practicing independently in one state may require supervision the moment a clinic opens across state lines.
This is where multi-state clinics often stumble. Internal policies don’t automatically adapt to state law, and assumptions travel faster than compliance reviews.
Clinics that scale successfully treat FPA as state-specific infrastructure, not a universal rule.
How Clinics Can Use Full Practice Authority Strategically
When aligned correctly, full practice authority allows clinics to:
- Expand access to care
- Reduce unnecessary physician bottlenecks
- Improve scheduling flexibility
- Support sustainable growth
The key is structuring roles, policies, and oversight in a way that reflects state authority while maintaining internal accountability.
This is why many clinic owners rely on ongoing regulatory guidance for clinic owners rather than reacting to enforcement or audit pressure later.
The Real Takeaway
Full practice authority changes how nurse practitioners may practice—but it doesn’t remove a clinic’s responsibility to structure care lawfully.
Clinics that understand how FPA works at the state level gain flexibility without exposure. Clinics that assume independence equals simplicity often discover risk only after someone external starts asking questions.
Understanding these distinctions early helps clinics grow with confidence—not correction.
How We Support Clinics Navigating Full Practice Authority

Full practice authority creates opportunity—but only when clinics understand how to structure it correctly.
We work with healthcare clinics to translate state scope of practice laws into clear, defensible operational models. That includes reviewing how nurse practitioners are integrated into care delivery, how authority and accountability are documented, and how clinic policies align with state requirements.
For clinics operating in full practice authority states—or expanding into them—this kind of upfront clarity helps avoid restructuring later under audit, payer review, or growth pressure.Our goal isn’t to slow clinics down. It’s to help clinics use the flexibility full practice authority offers without creating hidden compliance risk.




+ show Comments
- Hide Comments
add a comment