")
On paper, nurse practitioners often appear interchangeable across clinics.
They’re licensed. Experienced. Capable of diagnosing, treating, and managing patient care. But legally, their authority can change the moment a clinic crosses a state line.
That difference isn’t academic—it’s structural.
Nurse practitioner scope of practice laws are set at the state level, and for healthcare clinics, misunderstanding those rules can quietly affect supervision models, delegation decisions, billing workflows, and compliance exposure.
Who Needs to Be Paying Close Attention to This

If you own or operate a healthcare clinic that employs nurse practitioners, state scope of practice laws already shape your business—whether you’ve planned for them or not.
This matters for clinics of all types: primary care, specialty practices, outpatient facilities, and clinics expanding across state lines. It also applies when clinics adjust staffing models to improve access, reduce physician burden, or scale services efficiently.
NP authority does not follow the provider—it follows the state.
What This Means for Clinic Owners
Nurse practitioner scope of practice laws determine how independently NPs may practice and what level of physician involvement is required.
Depending on the state, these laws govern:
- Whether NPs may diagnose and treat independently
- Prescriptive authority, including controlled substances
- Requirements for physician supervision or collaboration
- Documentation and contractual obligations
These rules are not optional guidelines. They are enforced through licensing boards, payer audits, and regulatory review.
Understanding state-by-state nurse practitioner scope of practice is essential because clinics are evaluated on how authority is structured—not how well care appears to function day to day.
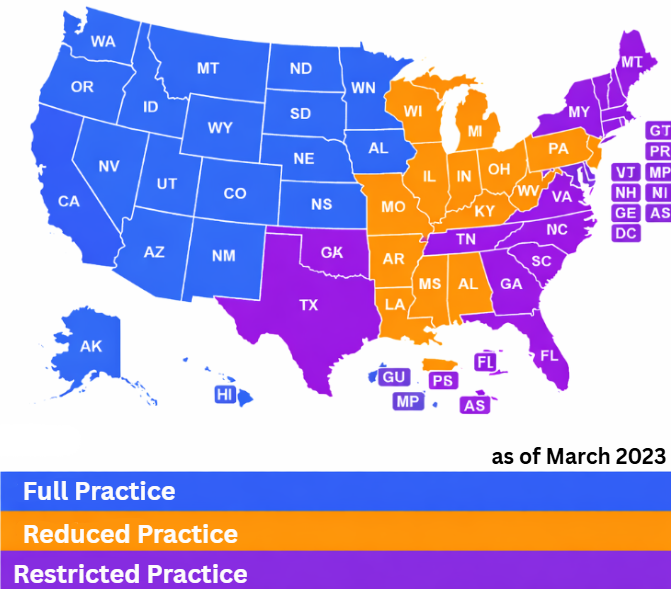
The Three Scope of Practice Models States Use
States generally fall into one of three categories.
Some states grant full practice authority, allowing nurse practitioners to evaluate patients, diagnose, treat, and prescribe independently under their own license. Clinics in these states have more flexibility in staffing and supervision design.
Other states follow a reduced practice model, where NPs can provide many services independently but must maintain a collaborative agreement with a physician for certain aspects of care.
Finally, restricted practice states require formal physician supervision or delegation for most or all NP activities. In these states, clinics must carefully document oversight and authority flow to remain compliant.
A clear breakdown of these models is maintained through scope of practice defined by healthcare regulation and updated regularly as laws evolve.
Why These Differences Matter Operationally
From a clinic’s perspective, NP scope of practice affects far more than job descriptions.
It influences:
- Staffing ratios and scheduling
- Supervisory structures and contracts
- Billing and reimbursement workflows
- Risk allocation within the practice
A staffing model that works smoothly in one state may require restructuring in another. Clinics that assume uniform NP authority across locations often discover compliance gaps only during audits or expansion planning.
This is where clinics benefit from building a defensible clinical structure that reflects state-specific authority rather than convenience.
Prescriptive Authority Is Often the Pressure Point
Prescriptive authority is one of the most regulated aspects of NP practice.
Some states allow broad prescribing authority, while others restrict controlled substances or require physician sign-off. These rules affect clinical flow, patient access, and liability exposure.
Professional standards governing nurse practitioner practice emphasize that prescriptive authority must align with both state law and clinic policy—misalignment between the two creates risk for the organization.
Why Clinics Get Caught Off Guard
Most clinics don’t ignore NP scope of practice intentionally.
They rely on experience, internal trust, or assumptions carried over from prior states. But when external scrutiny occurs—through payer review, licensing audits, or growth-related due diligence—those assumptions are tested against statute, not intent.
This is why many clinic owners rely on ongoing regulatory guidance for clinic owners rather than correcting issues after they’ve already drawn attention.
How Clinics Can Use NP Authority Strategically
When structured correctly, nurse practitioner authority can be a powerful asset.
Clinics that align staffing with state law can:
- Expand access to care
- Improve operational efficiency
- Reduce unnecessary physician bottlenecks
- Maintain defensible compliance positions
The key is designing models that respect legal boundaries while supporting clinic growth—not forcing authority where it doesn’t exist.
Contact a real council for you clinic now!
The Real Takeaway
Nurse practitioner scope of practice laws are not uniform—and that variability matters.
Clinics that understand how state laws define NP authority build stronger, more flexible care models. Clinics that assume consistency often discover limits only after someone external starts asking questions.
Understanding these rules early helps clinics grow with confidence—not correction.




+ show Comments
- Hide Comments
add a comment